|
Getting your Trinity Audio player ready...
|
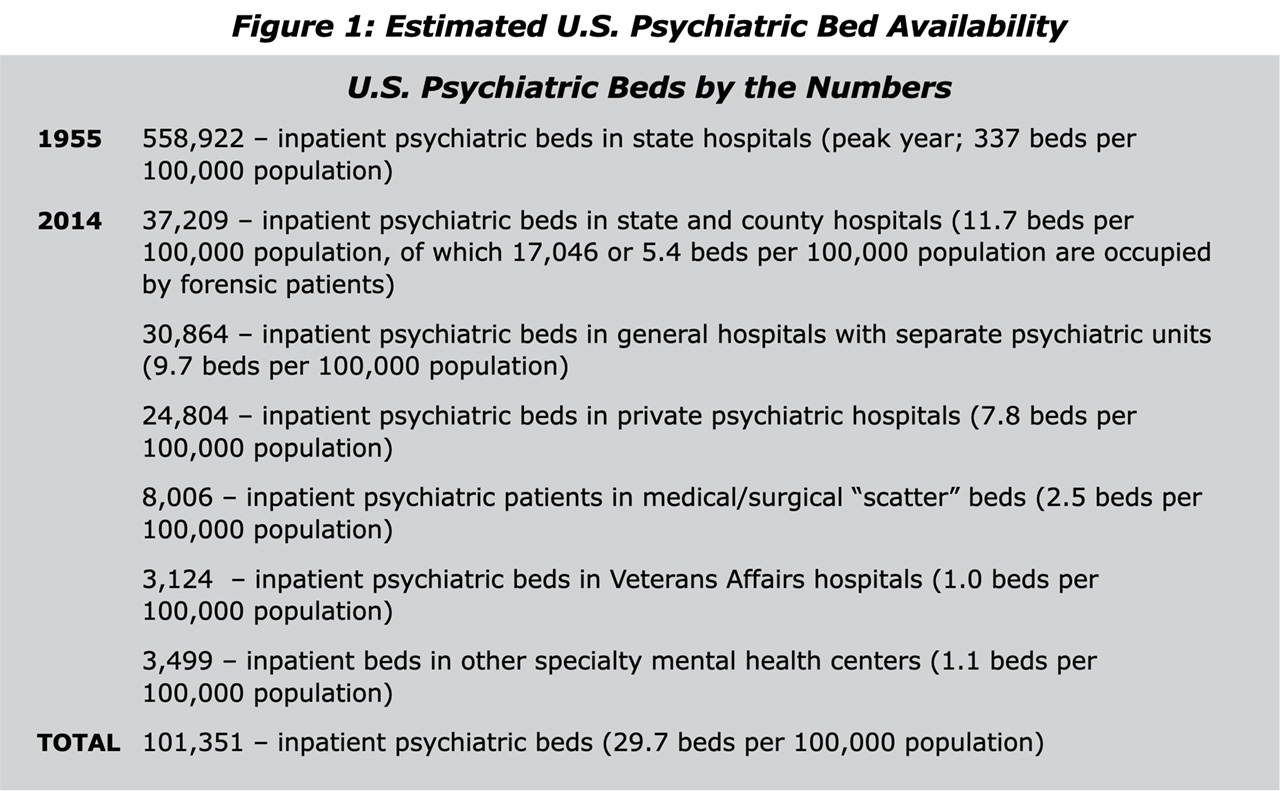
In 1955, the U.S. had more than 550,000 inpatient psychiatric beds.

“I think popular perceptions of inpatient mental health care gave political cover to the deinstitutionalization movement.” — Alice Feller, psychiatrist, advocate, and author
When legislators created Medicaid in 1965, they didn’t want the nation’s vast mental health network — along with its negative perception created by books and movies — to gobble up the new federal insurance dollars, says Alice Feller, psychiatrist, author, and mental health advocate.
By 2014, a comprehensive count of beds showed a little more than 101,000 inpatient psychiatric beds spread over differing types of facilities.
And, while Gov. Gavin Newsom’s recently passed Proposition 1 directs $6 billion in bonds to build more of the badly needed facilities, that decision in 1965 continues to limit access among the poor to mental health treatment.

Feller is the author of the book “American Madness: Fighting for Patients in a Broken Mental Health System,” published this year.
She attributes much of the decline in inpatient mental health beds to a legislative decision at the time to not include inpatient mental health treatment in Medicaid. That verdict is called the “institutions for mental disease exclusion.”
The IMD exclusion kept funding from going to facilities with more than 16 beds.
That drastic decline in the number of beds has forced many people facing mental health crises to deal with problems on their own or go to jail for a crime they committed while suffering from oftentimes treatable illnesses.
Legislators have more recently begun to recognize the need for expanded inpatient care, as Newsom and California voters did with Prop. 1. Still, there are many hurdles ahead.
Related Story: Newsom’s Prop 1 Promises to Build & Fund Mental Health Beds. But it ...
For example, the IMD exclusion still limits how those on Medicaid or in California, MediCal, can pay for services. And, Newsom’s CARE Act that allows courts to mandate mental health treatment will roll out later this year in Fresno County without additional funding.
“We’re all lobbying for the things that we need most in the worst way, particularly beds,” Feller said. “That’s acute care beds, acute hospital beds and then, subacute beds for people to get care and treatments and get ready for the next step down.”
Facility Treatment Should Be an Option, but It’s Hard to Access: Feller
The National Institute on Mental Health estimates 5.5% of the nation’s adults suffer from severe mental illness. Feller estimates 1% of the population suffers from schizophrenia specifically.
Not only do people with severe mental illness struggle to take care of themselves, they can also be a danger to others.
When Feller was in residency, she treated a woman with Capgras syndrome, which causes its sufferers to think that loved ones have been replaced by an imposter. This woman thought her son had been replaced by aliens.
“She killed him and then called the police because she couldn’t find her real boy. They finally found his body in a closet,” Feller said.
But Feller says early diagnosis and treatment can prevent those kinds of actions from happening. The difficulty comes in having resources available to provide that treatment.
1 in 8 ER Visits Involves Mental Health or Substance Abuse
One in eight emergency department visits involve a mental health or substance use condition, according to the National Alliance on Mental Illness. But with limited beds, emergency department staff often have to release patients because there’s no room in a treatment facility.
And police are limited in their response to emergency calls.
“When the desperate mother calls the cops because her son is on a rampage and has the knives out, (the cops) come to the house and they say, ‘well, there’s nothing we can do because he has shelter,’ ” Feller says.
The only alternative oftentimes is jail or prison.
Related Story: Mental Health by Mandate? Newsom’s Court-Ordered Care Debuts Monday
Many suffering from mental illness often praise the close care they can get in a specialty facility.
Feller says the perception is that people spend months or years in a facility, but more often it’s days or a couple weeks. But in a facility, doctors can see patients every day to ask how treatment is working and whether there is improvement. Staff is trained to work with mentally ill patients and help with recovery.
One woman Feller works with was convinced she could fly to the point she considered jumping off of a high place, Feller said. After inpatient treatment, that woman is now receiving training to become a peer counselor to others with mental illnesses.
“It’s completely different from being treated in the emergency room where you might get a shot of Haldol or something and be sent on your way,” Feller said.
Why Did Legislators Exclude Inpatient Mental Health Care from Medicaid?
The 19th Century saw movements to reform mental health care. By the 1940s and 1950s, many state hospitals were nearing 100 years old and needed significant repairs, according to a report from the National Association of State Mental Health Program Directors.
What’s more, World War II veterans returning from service with psychiatric conditions largely wanted to be treated closer to home rather than in institutions. The discovery of the medication Thorazine also made treatment at home more accessible.
Negative perceptions of institutional treatment also promulgated the move away from inpatient facilities.
After the publishing of 1961’s “The Myth of Mental Illness” by Thomas Szasz, it became common to hear that there was no such thing as mental illness, Feller said.
The 1962 book “One Flew Over the Cuckoo’s Nest” by Ken Kesey criticized mental health institutions and became even more popular after the movie in 1975.
In 1965’s Medicaid rules, individuals between 22 and 64 years old could no longer get reimbursed for treatment in psychiatric facilities with more than 16 beds under the IMD exclusion.
Public opinion played no small role in that decision, Feller said.
“I think popular perceptions of inpatient mental health care gave political cover to the deinstitutionalization movement,” she said.
Voters Authorized $6B in Facility Bonds, but Access for MediCal Patients Harder
California voters in March approved Proposition 1, which authorized $6 billion in bonds to create more inpatient mental health facilities across the state. But California has a lot of ground to make up.
Rates of serious psychological distress reaches 9.3% in the southern San Joaquin Valley, compared to 7.9% in the San Francisco Bay Area, according to a 2022 paper from Rand Health Quarterly. The 2022 study estimates the northern and southern San Joaquin Valley to be in the greatest need.
Researchers estimated a 4% growth in the need for beds in the San Joaquin Valley compared to the 1.7% growth needed statewide.
The Rand paper estimates California needs another 4,767 subacute and acute care psychiatric beds.
Authors of Prop. 1 say the bond will provide 4,350 housing units and 6,800 mental health and addiction treatment beds.
But the IMD exclusion still limits what services Medicaid or MediCal covers. Most people with private insurance can get inpatient care covered, but getting lower income people covered by state insurance requires a waiver still not approved in California.
In 2018, the U.S. Department of Health and Human Services introduced the waiver for the IMD exclusion, but that funding often comes at the cost of other federal reimbursement dollars, according to Ahmadreza Bahrami, division manager of public behavioral health with the Fresno County Department of Behavioral Health.
Fresno County has applied for the waiver through California, but the approval is still pending.
“The waiver also has significant limitations, so not all treatment setting types would apply,” Bahrami said.
Newsom’s CARE Act Rolls Out Locally With No Additional Funding
In 2023, seven California counties created CARE courts, including their plan for giving family members, care givers, and first responders the ability to send those needing mental health care before the courts to determine if they need treatment.
This year, the remaining counties will roll out their plans and processes.
The hope was to provide treatment for those who don’t know they need it. Those found by the courts to need treatment will get an individualized plan, which can include being in a locked facility.
Related Story: As CA Counties Hold Back Funds, Mental Health Providers Say They’re on ...
Some civil rights groups have questioned the constitutionality of committing people against their will. Others, including Feller, say people with severe mental illness often don’t know they’re ill.
Paying for mandated care will depend on the person’s insurance. Those with private insurance will be billed through their plans, said Bahrami. The county will have to take up the costs for those without insurance or MediCal with the county’s existing funding.
“It’s certainly somewhat hamstrung because it means the locality has to pay for it entirely,” Feller said. “We have Prop. 1 now, which should give us more money for this kind of thing. And we’re hoping — it’s supposed to fund more treatment facilities at all levels. But they’re kind of tiptoeing into that.”